Introduction
How to Deal With a Case Study
Case studies in Pathophysiology differ from those in basic physiology. Basic physiology case studies are designed to lead you through the consequences of ONE change in a system; you can usually identify a single cause for the client's problem and a single chain of events leading to the consequences.
In Pathophysiology, you are more interested in how a change in one system causes other systems to react, so the case study may contain several different chains of events.
You can navigate through this tutorial using the buttons at the top of the screen.
The tutorial will ask you questions. Click on your chosen answer to see feedback; click the answer again to make the feedback disappear. When you're finished with one page, click the navigation button for the next page to move ahead.
Now let's go to page 1 and get started!
Page 1
Basic Model of Pathophysiology Case Studies
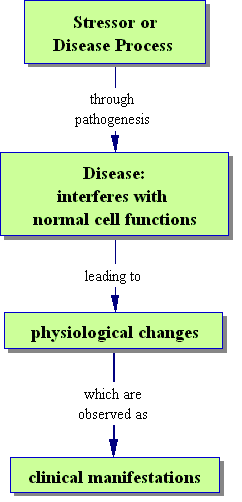
A thorough analysis will start with the stressor or disease, and how it damages the body. Then you'll infer what problems this kind of damage will cause, and relate them to clinical manifestations -- signs and symptoms.
With this analysis, you should be able to explain what's going on to the patient, and make clinical decisions like what signs to watch for.
Page 2
You should be able to write a clear paragraph about how the stressor damages cells. It's important to think about this at the CELLULAR level -- that is, what chemical components of the cells are altered and how do they affect cell function -- because most of our medicines are chemicals, and that's the level on which they work.
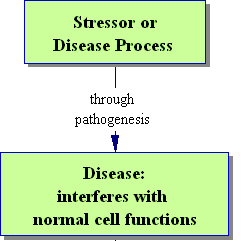
A good way to prepare for solving case studies would be to make sure that for each disease, you have a brief and clear statement of its pathogenesis in your notes. This is also a good place to put the drugs used to treat it, as you can explain just which step in the pathogenesis each drug affects.
Page 3
In Physiology, you may have talked a little bit about how the client experiences a change in physiological function. In Pathophysiology, this concept becomes key -- because the clinical manifestations are what bring the client in to see the doctor, and are what the doctors and nurses use to assess the client's condition.
Many clinical manifestations can be inferred directly from the changes in function. You will also learn some general patterns of clinical manifestations associated with common situations like systemic inflammation, hypoxia, and the generalized stress response. Look for these patterns in a case study; they will allow you to break it apart into manageable pieces.
Page 4
Let's try it!
Mrs. K was in a motorcycle accident and suffered a broken leg with abdominal injuries. She lost a great deal of blood.
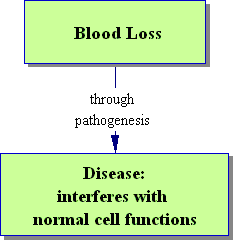
Why is this a problem for Mrs. K at the CELLULAR LEVEL?
Page 5
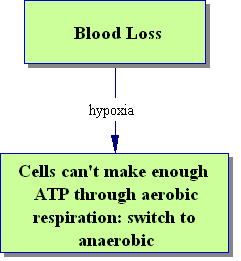
Hypoxia is the major problem caused by blood loss.
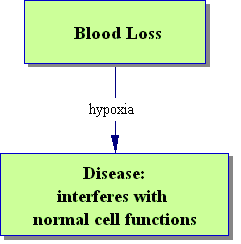
But why does it matter? Why can't her cells do fine without Oxygen? Choose the process for which cells need the most oxygen.
Page 6
If her cells can't make ATP, Mrs. K will suffer decreases in cell function.
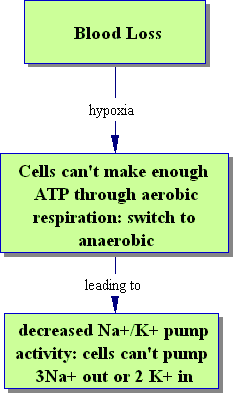
What is one of the functions that will be affected?
Page 7
If she can't run the Na+/K+ pump, Mrs. K can no longer control water and ion balance in her cells. Less Na+ will be pumped out and less K+ will be pumped in.
What might happen??
Page 8
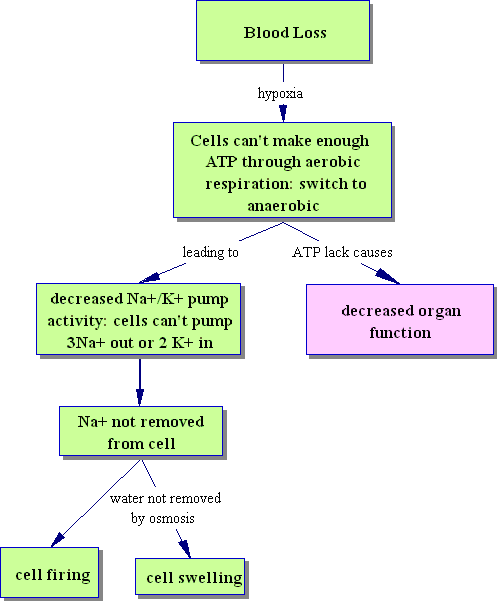
One of the first consequences of hypoxia is that cells begin to swell up with water. If this becomes severe enough, they may begin to burst.
Na+ builds up in nerve and muscle cells, so they may begin to fire uncontrollably -- which means that they use even more of their ATP, and have even less to run their Na+/K+ pumps with. This is why lack of Oxygen to the brain or heart muscle has such severe consequences, so quickly.
If Mrs. K's hypoxia were to continue, she could develop many different problems, because cells in every part of the body would suffer a decrease in function due to their inability to make enough ATP.
These new diseases would be called COMPLICATIONS.
Page 9
Let's look at what happens next in Mrs. K's case, to see what COMPLICATIONS she may be developing:
Mrs. K was in a motorcycle accident and suffered a broken leg with abdominal injuries. She lost a great deal of blood. Over the next two days in the hospital, Mrs. K did not produce any urine and the levels of nitrogenous wastes in her blood increased. She also developed an irregular heartbeat with changes in her EKG. What is one COMPLICATION Mrs. K is developing?
Page 10
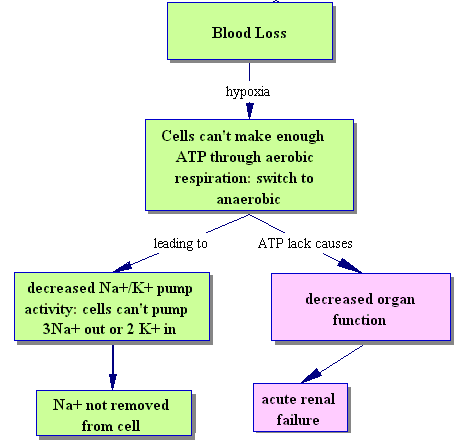
Mrs. K's inability to produce urine and increased levels of nitrogenous wastes in her blood indicate renal failure. But she also developed an irregular heartbeat with changes in her EKG.
What is another COMPLICATION we should add to this flow chart?
Page 11
Good work! Mrs. K's clinical manifestations indicate trouble with both her kidneys and her heart.
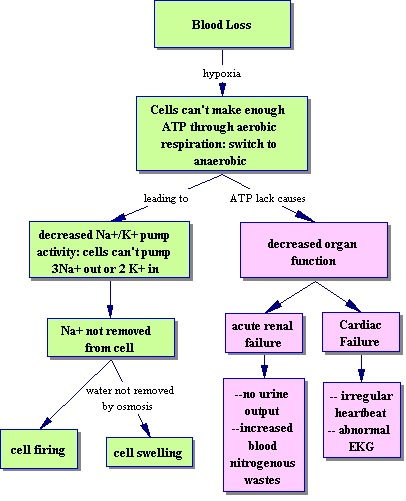
Notice that in this case study, although you know what the underlying problem is with Mrs. K's cells -- lack of ATP and inability to run the Na+/K+ ATPase -- that's not what you actually see in the client. Mrs. K presents with clinical manifestations of the COMPLICATIONS caused by her hypoxia.
Complications are a major problem in Pathophysiology and in medicine. You can spend lots of time and effort treating emergencies caused by complications; obviously, this won't do the client as much good as solving the underlying problem!
This is why you should never ignore the pathogenesis of the disease in your analysis, no matter how much more exciting or obvious the complications seem. Your ultimate goal is to treat the client's basic problem so that the complications will never arise. You can clearly see that if Mrs. K's blood loss had been taken care of right away, or if she had never developed hypoxia, or if she had been able to produce ATP in spite of her hypoxia, she might never have developed either renal failure or cardiac failure.
But clients' underlying problems don't always get this kind of immediate treatment. That means that somebody who is working closely with the client needs to know which complications might develop, and how to tell they are happening.
Page 12
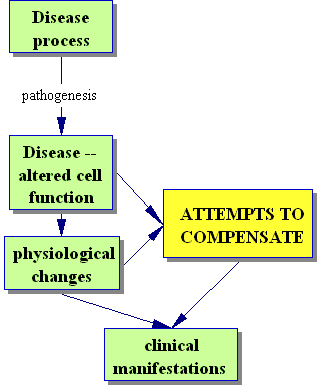
Because the changes in cell function and physiology could lead to catastrophic complications, the body will try to compensate for those changes.
This means that a lot of the clinical manifestations you see in the client may not be caused by any disease at all: they may be indications of a normal compensating mechanism, or Adaptation.
It's essential for you to be able to pick out the signs of a disease, that must be treated, from the signs of a compensating response that might be keeping the client alive. If you were to give a treatment that reduced the compensating response, you might make the client's situation worse instead of better! In addition, the signs of compensation will tell you that the patient's body thinks there is a problem -- and it knows better than you do.
The major compensating response in Pathophysiology is the GENERALIZED STRESS RESPONSE. A good initial question to ask about any case is, "Is the GSR on? If so what signs and symptoms are caused by it?" In this response to pain, fear, stress, hypoxia, or decreased blood pressure, four things happen: the Sympathetic Nervous System turns on, the Renin-Angiotensin-Aldosterone pathway turns on, and Corticotropin Releasing Hormone and Antidiuretic Hormone are secreted by the hypothalamus. You should be familiar with these pathways from Physiology. If not, you can review some of them at these links: otherwise, move on to the next page and apply your knowledge of the GSR to Mrs. K's case.
NEW RAAS tutorial
NEW Sympathetic System review
NEW CRH release
Page 13
Mrs. K suffered a broken leg and abdominal injuries in a car accident.
Click on the clinical manifestations caused by her Sympathetic Nervous System.
When she was brought into hospital she presented as a forty-three year old white female, anxious and
restless, with a
rapid pulse and
increased respiration rate.
She was pale with
cold, clammy skin. Pupils were
dilated and reactive.
Blood pressure was 125/65 mm Hg and blood tests showed
increased blood glucose and decreased hematocrit The client had
no bowel sounds and produced
no urine during her 5 hours in the emergency room.
Page 14
Mrs. K suffered a broken leg and abdominal injuries in a car accident.
Click on the clinical manifestations caused by her Renin-Angiotensin-Aldosterone System.
When she was brought into hospital she presented as a forty-three year old white female, anxious and
restless, with a
rapid pulse and
increased respiration rate. She was
pale with
cold, clammy skin. Pupils were
dilated and reactive.
Blood pressure was 125/65 mm Hg. Blood tests showed
increased blood glucose and
decreased hematocrit. Client had
no bowel sounds and produced
no urine during her 5 hours in the emergency room.
Page 15
Mrs. K suffered a broken leg and abdominal injuries in a car accident.
Click on the clinical manifestations caused by her Corticotropin Releasing Hormone or Antidiuretic Hormone.
When she was brought into hospital she presented as a forty-three year old white female, anxious and
restless, with a
rapid pulse and
increased respiration rate. She was
pale with
cold, clammy skin. Pupils were
dilated and reactive.
Blood pressure was
125/65 mm Hg. Blood tests showed
increased blood glucose and
decreased hematocrit.
Client had
no bowel sounds and produced
no urine during her 5 hours in the emergency room.
Page 16
Here's an overall flow chart of Mrs. K's case. Notice the three major components:
1. Her initial disease and pathogenesis (green), with their clinical manifestations
2. Her complications (pink), with their clinical manifestations
3. Her compensatory responses (yellow), with their clinical manifestations
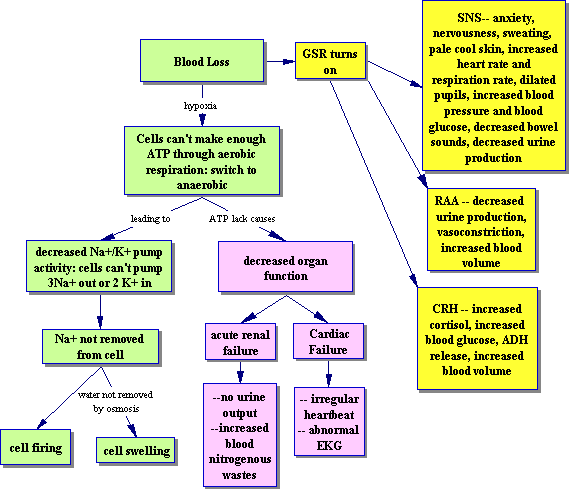
As well as going through the steps of analysis of a case study, this tutorial has shown you the pathways of Compensated Shock. Mrs. K suffered from decreased blood volume, but her GSR was able to compensate for it.
I left something out of this flow chart; I didn't distinguish which of those SNS signs were caused by which receptors. You should be able to add this in, so you can predict what will happen if any of those receptors are blocked (for instance, by meds).
This is the end of the case basics tutorial. Happy studying!